E-Mail Edition Volume 13 Number 1
Published Winter, 2016
Published by Piccadilly Books, Ltd., www.piccadillybooks.com.
Bruce Fife, N.D., Publisher, www.coconutresearchcenter.org
If you would like to subscribe to the
Healthy Ways Newsletter
Contents:
-
Protect and Restore Your Vision with Coconut Oil
-
New Study Shows Low-Fat Diets Don’t Work
-
Warning: Medicines Your Child Shouldn’t Take

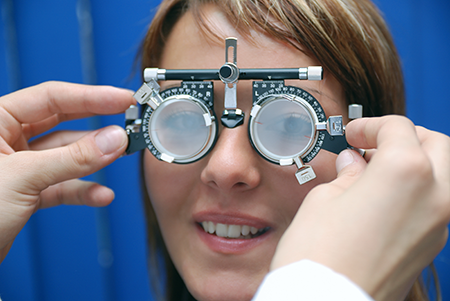
Protect and Restore Your Vision with Coconut Oil
If you are concerned about losing your eyesight to diabetic
retinopathy, cataracts, glaucoma, macular degeneration, or other
age-related degenerative eye disorders, coconut oil may provide
a solution for you.
Vivian was diagnosed with
diabetes 20 years ago at the age of 58. "To be quite honest," says
Vivian, "when I was first diagnosed I don’t really remember what I was
told. I think I was so shocked to realize I was falling prey to
diabetes, a disease I thought I would never get. I was always a healthy
person&mdashnever sick." Today Vivian manages her condition with four
injections a day: two of insulin and two of Byetta—a drug to help
control blood sugar.
Ten years ago, she was
diagnosed with diabetic retinopathy—a degenerative eye disease brought
on by her diabetes.
"I was not
prepared for vision problems," says Vivian. "The doctor who first
treated me for diabetes didn’t mention that I needed to take care of my
eyes. He didn’t suggest that I should go and see an ophthalmologist
every year for a checkup. I don’t think too many people know that you
can lose your vision to diabetes. I’ve heard of people who have had legs
and other limbs amputated, but I didn’t know it could affect your eyes."
Retinopathy can develop
without any noticeable symptoms. The retina can be damaged before the
person notices any change in vision. Blurred vision may occur when the
retina swells from leaking fluid. At first, a few specks of blood, or
spots may also interfere with vision. Sometimes, without treatment, the
spots clear, and the person will see better. However, bleeding can
reoccur and cause severely blurred vision and scaring. If it advances,
risk of permanent vision loss is high. Despite taking medications to
control her blood sugar, every time Vivian eats too much
carbohydrate-rich food her vision becomes blurry, indicating leakage and
swelling in her retina. Blurred vision is often one of the first signs
of diabetes.
Diabetes is a major cause of
disability leading to blindness, lower-limb amputation, kidney disease,
and nerve damage. According to the American Academy of Ophthalmology
people with diabetes are 25 times more likely to become blind than
people without the disease. Currently 29 million people (9.3 percent of
the population) in the United States have diabetes. Over 8 million are
living with diabetes but are unaware of it. More than 26 percent of all
adults age 65 and older have diabetes: that’s one out of every four
older adults! But it’s not just an old-age disease; over 200,000 people
under the age of 20 have been diagnosed with the disease as well. There
are many more people, 86 million age 20 years and over, who are
pre-diabetic. All of these people are at risk of developing visual
problems at some point in their lives.
Diabetes not only causes
retinopathy but also increases the risk of developing other visual
problems such as cataracts, glaucoma, and macular degeneration. People
with diabetes develop cataracts at an earlier age, and are nearly twice
as likely to get glaucoma compared to non-diabetics.
Diabetes occurs as a result
of the body’s inability to properly regulate blood sugar. When we eat a
meal, much of the food is converted into glucose, or blood sugar, and
sent into the bloodstream. When blood sugar levels rise too high, the
body can be thrown into a panic, metabolically speaking. The pancreas
releases insulin into the bloodstream to shuttle glucose into the cells
and lower blood sugar levels. However, if blood sugar is not normalized
in a reasonable amount of time, cells and tissues become damaged. This
is what happens in people with diabetes.
Ninety percent of all
diabetics are type 2 or insulin resistant. Their cells have become
unresponsive or resistant to the action of insulin so blood sugar has a
harder time being transported into the cells. As a consequence, blood
sugar levels remain elevated for extended periods of time. You don’t
have to be diabetic to develop problems. Even pre-diabetics are at risk.
Any elevation of blood sugar is harmful to the eyes.
When insulin resistance is
severe, it is classified or diagnosed as diabetes. Diabetes is diagnosed
when fasting blood sugar—the blood glucose levels after an 8-12 hour
fast—reaches 126 mg/dL (7 mmol/L) or more. In a healthy individual
fasting blood sugar levels are generally no greater than 90 mg/dL. The
higher the blood sugar level is, the greater the damage being done.
Chronic fasting blood sugar levels over 90 mg/dl increase your risk of
degenerative eye disease.
If you have problems with
cataracts, glaucoma, macular degeneration, or any other age-related eye
disorder then you are most likely insulin resistant to some degree. For
example, the higher a person’s blood sugar is, the greater the risk of
cataract. Researchers at Yale University studied the effect of three
diets—high-carb, high-protein, and high-fat—on the incidence of cataract
in diabetic rats. Development of cataracts was highest in the rats fed a
high-carb diet; a lesser incidence was observed in the high-protein fed
animals, while no cataracts developed in rats fed a high-fat diet.1
Although all the rats in this study were diabetic, their blood sugar
levels determined the severity of cataracts they developed. The higher
the blood sugar levels, the greater the incidence of cataract. When
blood sugar was controlled by a high-fat, low-carb diet, no cataracts
developed. This effect is not seen just in lab animals, in humans better
blood sugar control has shown similar results.2
Whether you are diabetic or
not, eating a high-carb diet will elevate blood sugar and keep it
elevated for extended periods of time and increase the risk of damaged
to the eyes. Scientists working for the US Agricultural Research Service
tracked 471 middle-aged women during a 14 year period. The researchers
found that women in the study whose average carbohydrate intake was
between 200 and 268 grams per day, which is typical for most normal
weight women, were 2.5 times more likely to get cataracts than the women
whose intake was between 101 and 185 grams per day. Although the
consumption of 101 to 185 grams per day is lower than average, it is not
considered low-carb. Low-carb diets generally include no more than 100
grams of carbohydrate a day and very low-carb diets restrict it to less
than 25 grams daily. So even a modest reduction in carbohydrate intake,
and corresponding drop in blood sugar levels, can significantly reduce
risk of cataracts.3
Fasting blood sugar measures
the glucose levels at the time of testing. Another way of measuring
blood sugar that gives an average over the previous three months is the
A1C test. Researchers at the University of Oxford found that type 2
diabetics who lower their A1C level by just 1 percent can reduce their
risk of cataracts by 19 percent.
6 Even a small decrease in
average blood sugar can make a big impact on eye health.
A study out of Tufts
University in Boston showed that eating foods with a glycemic index
above average is associated with a 49 percent increase in advanced
macular degeneration.4 The glycemic index is a measure of how
quickly certain foods raise blood sugar levels. Those that raise blood
sugar levels the most, like bread and sugar, are the most detrimental.
Dr. Allen Taylor, the lead researcher in this study, said that the
results found that at least 1 in 5 cases of advanced age-related macular
degeneration (the only eye disease evaluated in the study) would likely
have been prevented entirely by consuming a lower-carb diet.
You may be at risk of developing an age-related eye disease, even if you are not diabetic and have no known visual difficulties; we are all at risk. Degenerative eye diseases don’t appear overnight. They take years, even decades to develop. Glucose metabolism becomes abnormal one to two decades before type 2 diabetes is diagnosed.5 In the meantime, the damage that can be done could be extensive before any symptoms become noticeable. Since no pain or sudden changes in vision are noticed, the gradual loss of sight is not easily recognized until
The
cataract started bothering me with a blurred film on my left eye. So
after reading [The Coconut Oil Miracle], we purchased a coconut from
Wal-Mart and my husband drilled a hole to drain and I strained the water
through sterile gauze and used an eye dropper to instill about three
drops in my left eye then covered with a hot wash cloth for ten minutes.
I took off the washcloth and nothing had changed. However, the next
morning the eye was clear as a bell and has been ever since!!!
Dolores/DJ

Stop Vision Loss Now
by Dr. Bruce Fife
substantial damaged has occurred. Waiting until symptoms appear may be
too late.
A dietary approach is much
better and doesn’t require drugs. Even if you are severely diabetic you
can get your blood sugar under control using a low-carb, coconut
oil-based diet. A low-carb diet can help control blood sugar levels.
Coconut oil, in addition to helping with blood sugar, can reverse much
of the damage caused by chronic high blood sugar.
Coconut oil can work wonders
in alleviating symptoms associated with insulin resistance. Studies show
that the medium chain fatty acids (MCFAs) in coconut oil improve insulin
secretion and insulin sensitivity.6 This means, coconut oil
can improve cell sensitivity to insulin and lower blood sugar levels. In
addition, coconut oil can help keep blood sugar from spiking after
meals. When added to foods, coconut oil slows down the absorption of
sugar into the bloodstream, thus moderating blood sugar levels.
Insulin resistance impedes
glucose transport into the cells, essentially starving the cells,
causing them to slowly degenerate and die. This is what leads to the
major complications associated with diabetes. Blood vessels and
capillaries degenerate and become leaky. Circulation is hampered. This
leads to diabetic neuropathy (loss of feeling) in the feet and legs,
which could progress to foot ulcers, gangrene, and amputation. It could
also lead to a poor circulation to the eyes, the development of
retinopathy, and vision loss.
Coconut oil can stop this
degenerative process and restore the health and function of damaged
blood vessels and capillaries, in the eyes. Unlike glucose or long chain
fatty acids, MCFAs are not affected by insulin resistance. They do not
require insulin to enter the cells. They easily diffuse across the cell
membrane to provide the cells in the eyes with nourishment, allowing the
blood vessels and capillaries to repair themselves and for proper
circulation to be restored.
It has been estimated that
up to 80 percent of the population has some level of insulin resistance
(fasting blood sugar above 90 mg/dl) and that their cells are not
absorbing glucose effectively. As a consequence, blood vessels and
capillaries throughout the body are being damaged, which increases the
risk of age-related eye disorders such as cataracts, glaucoma, macular
degeneration, and diabetic retinopathy.
For this reason, it is a
good idea to have your eyes examined periodically. Also, have your
fasting blood glucose levels checked every few years. If your blood
sugar is high, you can take steps now to correct the problem and greatly
reduce your risk of experiencing vision loss later on.
For a more complete
discussion on how coconut oil combined with a proper diet can prevent,
stop, and even reverse degenerative eye disorders see my new book
Stop Vision Loss Now!
References
-
Rodriguez, RR and Krehal, WA. The influence of diet and insulin on the incidence of cataracts in diabetic rats. Yale J Biol Med 1951;24:103-108.
-
The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Research Group. N Engl J Med 1993;329:977-986.
-
Chiu, CJ, et al. Carbohydrate intake and glycemic index in relation to the odds of early cortical and nuclear lens opacities. Am J Clin Nutr 2005;81:1411-1416.
-
-
-
Stratton, IM, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-412.
New Study Shows
Low-Fat Diets Don’t Work
If you’ve ever tried to lose weight on a low-fat diet you know how difficult it can be. Not only is total food intake severely restricted, but every morsel of fat is to be avoided at all costs. Fatty chicken skin is removed, any fat on lean cuts of meat is carefully trimmed off, fat-free egg whites are chosen over whole eggs and low-fat and non-fat milk, yogurt, and cheese become your preferred choice. You carefully count every calorie that passes through your lips. Foods devoid

of fat taste
bland and unappetizing, so they are often enriched with additional sugar
to make them more palatable.
This was the
conclusion of a recent study published in the
American Journal of Public Health. Researchers at King’s College in
London found that the chance of an obese person attaining normal body
weight is 1 in 210 for men and 1 in 124 for women, increasing to 1 in
1,290 for men and 1 in 677 for women with severe obesity. The findings,
reveal that current weight management programs focusing on low-fat
dieting and exercise are not effective in tackling our growing
overweight epidemic.
The research,
funded by the National Institute for Health Research (NIHR), tracked the
weight of 278,982 participants (129,194 men and 149,788 women) using
electronic health records from 2004 to 2014. The study looked at the
probably of obese patients attaining normal weight or a 5 percent
reduction in body weight; patients who received bariatric surgery were
excluded from the study. A minimum of three body mass index (BMI)
records per patient was used to estimate weight changes.
Body mass
index is a numerical value derived from the weight and height of an
individual. BMI is a much more accurate means to measure how fat or thin
a person is than by weight alone. The BMI is an attempt to quantify the
amount of fat, muscle, and bone a person has. A tall lean person can
weigh a lot more than a short fat person, so height is a critical
component in judging a person’s mass.
BMI is used to
assess how much a person’s body weight departs for what is considered
normal or desirable for his or her height. BMI between 18.5 and 25 is
considered normal or healthy. Less than 18.5 indicates underweight. More
than 25 signifies overweight. A person is considered obese if BMI is 30
or more and severely obese if the value is 35 or greater.
The most
recent figures on obesity in the USA say that 39 percent of the
population is now obese. America is not alone. The obesity epidemic is
felt worldwide. The waistlines of people all over the world are
expanding.
What is your
BMI? You can calculate your BMI using the following formula:
BMI =
weight (kg) ÷ height (m)2
If you use
pounds and inches you need a conversion factor of 703 and the formula
is:
BMI =
weight (lb) ÷ height (in)2
X 703
The
researchers in this study found that for those people who achieved 5
percent weight loss, 53 percent of them regained this weight within 2
years and 78 percent regained their lost weight within 5 years. These
results correlate with previous observations that had estimated that as
many as 95 percent of those people who go on low-fat diets to lose
weight regain all their weight after 5 years.
Overall, only
1,283 men and 2,245 women in the study with a BMI of 30-35 reached their
normal body weight, equivalent to an annual probability of 1 in 210 for
men and 1 in 124 for women; for those with a BMI above 40, the odds
increased to 1 in 1,290 for men and 1 in 677 for women with severe
obesity. The study concluded that current obesity treatments are failing
to achieve sustained weight loss for the vast majority of obese
patients.
Dr. Alison
Fildes, one of the authors of the study, said, "Losing 5 to 10 percent
of your body weight has been shown to have meaningful health benefits
and is often recommended as a weight loss target. These findings
highlight how difficult it is for people with obesity to achieve and
maintain even small amounts of weight loss."
The standard
approach to treat overweight and obesity is to go on a low-fat, calorie
restricted diet and to increase physical activity. This approach is
based on the outdated theory that all calories are the same—the source
of the calorie has no effect. Lowering total calories will result in
weight loss regardless of the type of food consumed. Fat contains more
than twice as many calories per gram as carbohydrate or protein.
Consequently, most weight loss diets focus on reducing the fat in the
diet to allow as much carbohydrate and protein as possible. This
approach has proven to be a dismal failure.
Removing fat
from the diet has doomed these diets to fail. The reason is that a
healthy amount of fat is necessary in the diet to achieve optimal health
and weight. There are several reasons for this, let me mention just
three:
-
Fat satisfies hunger better than carbohydrates and protein. Fat slows down digestion so that foods remain in the stomach longer, extending the feelings of satisfaction and staving off hunger longer. Although fat supplies more calories than carbohydrate and protein, its effect on curbing hunger and discouraging overeating and snacking more than makes up for it by reducing total calorie intake.
-
-
Our bodies need fat. Every cell in the body needs fat. It is a major structural component of the body. It is also needed to make hormones and enzymes. Although our bodies can make fat from carbohydrate and protein, it cannot make enough on its own for optimal health. It needs fat in the diet. If the body does not get enough dietary fat, it activates fat producing enzymes that convert other foods into fat. When we eat enough fat, these fat producing enzymes are down regulated or switched off. In other words, the less fat you eat, the more fat your body makes and packs away into your fat cells. The more fat you eat, the less fat your body makes and the less fat that will wind up hanging around your waist, hips, and thighs.
One of the
main reasons why we are experiencing an obesity epidemic today is
because for the past 30 years or so we have been told to avoid fat and
eat lean. Weight loss diets stress the removal of fat from our
plates—just the opposite of what you should be doing to lose weight.
Coconut oil is an ideal fat for weight loss as it has been shown to
satisfy hunger and promote body fat reduction.
If you want to
lose excess weight, forget the typical low-fat diets. You will have far
greater success eating more fat in conjunction with a low-carb diet.
Reference:
Fildes, A, et al. Probability of an obese
person attaining normal body weight: cohort study using electronic
health records. American Journal of Public Health 1015;e1
DOI;10.2105/AJPH.2015.302773.
The Coconut
Ketogenic Diet
by Dr. Bruce Fife
Warning: Medicines Your Child Shouldn’t Take
Many medications just aren’t worth the risk. Does your child take any of
these dangerous drugs?
By Fredelle Maynard
The pharmacist was right.
Jason’s doctor knew the benefits of tetracycline, but he was ill-informed
about its side effects. Fortunately, the child’s mother consulted a second
doctor who prescribed penicillin—and Jason’s impetigo was cleared up without
ill effects. But not all children are so lucky. Many are given drugs that
are inappropriate, unnecessary or harmful to their health. A Boston hospital
study reports adverse drug reactions in 16.8 percent of child patients.
Depending on the age of the
child, the effects of a wrong drug range from the relatively mild (rashes,
nausea, vomiting) to the potentially serious and life-threatening
(gastrointestinal bleeding, convulsions, and coma). Excessive doses of some
toxic drugs can produce brain damage and death.
Why does this dangerous
situation exist? Doctors are human. They may be under pressure, exhausted,
distracted, even negligent. Like the physician who treated Jason, they
sometimes make mistakes. In addition, distraught parents often plead with
doctors to "do something" for a sick child. As Dr. Robert Issenman, director
of ambulatory pediatrics at Canada’s McMaster University Medical Center put
it, "A doctor may, against his deepest convictions, offer drugs to relieve a
child’s discomfort and ease parents’ anxiety."
Another problem, according
to Dr. Stuart MacLeod, chief of pharmacology at Toronto’s Hospital for Sick
Children, is our practice of acting swiftly to relieve symptoms. If a child
has diarrhea, nausea, fever, or pain of any kind, we seek an instant remedy
in the medicine cabinet. The trouble with such well-meaning intervention is
that it ignores—and may frustrate—the symptoms’ natural functions.
Diarrhea and vomiting are
the body’s way of expelling noxious substances. And fever may serve a useful
purpose—improving blood circulation, strengthening the immune defenses, and
reducing the spread of infection. (Except in infants under four months,
temperatures up to 104° F are usually well tolerated.) Pain is also an
important signal. Using drugs to mask it may allow a serious underlying
problem to develop undetected.
What’s the parent of a sick
child to do? First, says Dr Issenman, be aware that "the vast majority of
children’s illnesses are natural processes from which the patient will
recover without much intervention on the doctor’s part." It’s also important
to recognize, says Dr. MacLeod, that "no drug is absolutely safe for all
individuals under all circumstances." And children are especially
susceptible to the ill effects of medication.
Drugs can and do save lives,
of course. Often the benefits clearly outweigh the risks. It’s important,
however, for parents to understand when medication is appropriate for
children and which drugs may be dangerous to their health.
10 Riskiest Drugs for Children
Tetracycline. Causes
mottling and discoloration of the permanent teeth and nails in children
under eight. It can also hamper bone growth and produce intestinal
discomfort and liver damage. Because of its effect on teeth and bones, it is
not recommended for children under 12.
Ampicillin. A semisynthetic
penicillin that can be fatal to anyone allergic to penicillin, it can also
cause nausea, rash, diarrhea, vomiting, anemia, and inflammation of the
mouth. It should be used only for bacterial infections; in rare cases it can
produce deterioration of the bone marrow. (Amoxicillin is similar in
effectiveness but less likely to cause trouble.)
2. Antidiarrheals. Lomotil, once widely prescribed for diarrhea
resulting from a short-lived viral infection, is definitely not for
children. Side effects include bloating, constipaltin, loss of appetite,
blurred vision, drowsiness, fast heartbeat, and shortness of breath among
other things. Entero-Vioform and Diodiquin, sold over-the-counter in foreign
countries for traveler’s diarrhea, have been linked with irreversible nerve
and eye damage and should never be given to children.
3. Antihistamines. These drugs are effective against allergies,
but of limited help with cold symptoms, for which they are often prescribed.
Although generally safe in recommended doses, they do produce adverse
effects, including drowsiness, dizziness, blurred vision, insomnia, loss of
appetite, and occasionally even convulsions. Children under six should take
them only on a doctor’s advice—and should not play on jungle gyms, ride
bikes or climb trees while on them.
4. Aspirin.
Long the drug of choice for pain, fever, inflammation, headache, and
toothache, aspirin is now used more cautiously with children. It should not
be given to anyone under 10 unless prescribed by a doctor, because even
small doses can cause rashes, bleeding and intestinal upsets. In excessive
amounts, says Dr Frederick Lovejoy of Boston Children’s Hospital, aspirin
makes a child "breathe too fast, too hard; the whole internal chemistry goes
out of whack." Aspirin given during viral infection, such as the flu or
chicken pox, can lead to the life-threatening Reye’s syndrome.
5. Diaper Rash Preparations. When the skin surface is broken,
as in diaper rash, any chemical may be absorbed into the bloodstream and
affect the infant’s immature nervous system. (In the past, the unrestricted
use of boric acid powder proved fatal.) The American Pharmaceutical
Association cautions against hydrocortisone cream for diaper rash and says
that "the general use of any medication for a baby’s skin is questionable."
6. Growth Hormones. Human growth hormone (hGH) therapy was
developed for children whose growth had been severely curtailed by chronic
disease or a genetic defect. But parents of normal healthy short children
may ask their physicians about the "miracle" drug.
Growth-hormone treatment is
painful and protracted, requiring intramuscular injections three times a
week for two or more years. If administered to children who are not hGH
deficient, it may cause diabetes, hypertension, coronary-artery or
cerebrovascular disease—and it may not work. The American Academy of
Pediatrics recommends that the therapy be limited to children with hormone
deficiency.
7. Imipramine (Tefranil). Used to control bedwetting,
imiparamine has been touted as highly successful, with minimum
disturbance—psychological or physical.
Critics
point to evidence that the drug produces no significant permanent result;
when it’s discontinued, the child frequently reverts to nighttime wetting.
Possible side effects listed by the manufacturer include hallucinations,
nightmares, heart palpitation, hypertension, blurred vision, swelling of the
face and tongue, skin rashes, nausea, diarrhea, dizziness, irritability, and
jaundice. Long-term effects can hamper normal growth and development.
This amounts to overkill for
a problem that time usually solves. The greatest danger is accidental
overdose; tragic accidents have involved children who believed that more
means fast relief. One seven-year-old who‘d made nighttime progress with
imipramine wet his pants at school and attempted an all-out attack on the
problem. He took 40 tablets and died in a coma.
8.
Laxatives. All of those
pleasant-tasting potions for stimulating the bowels are risky for children.
So is caster oil, which can cause violent cramping and dangerous loss of
water and essential body salts. Mineral oil can impair absorption of
vitamins and other nutrients—and can be aspirated into the lungs of children
under six. Doctors also frown on suppositories for stimulating the bowels.
9. Ritalin.
A stimulant that paradoxically calms behavior while reviving up the heart
rate and metabolism. Ritalin is used to treat hyperactive children. Requests
for the drug often come from teachers who find certain students hard to
manage—and from parents exhausted by a child who throw tantrums, resist all
control, won’t sit still, and can’t sleep. But Dr. Sydney Walker, a
California neuropsychiatrist who sees many hyperactive children in his
practice, is adamantly opposed to use of the drug. "I have never prescribed
stimulants, and I never will." He says. He points out that hyperactivity is
not a disease but "a constellation of signs and symptoms that can occur for
various reasons." A child labeled hyperactive may, in fact, have a heart of
glandular problem, a calcium deficiency, be prediabetic, or suffer from
mild, almost undetectable brain seizures. In none of these cases would
Ritalin do the slightest good. In some, it would mask symptoms needing
attention.
Ritalin should never be a
first-line treatment, say Dr. Wendy Roberts, a specialist in learning
disorders at Toronto’s Hospital for Sick Children. And it should not be used
until sophisticated testing has determined that the child has the form of
hyperactivity that responds to drug treatment. Although Ritalin does reduce
frenetic activity in some children and can promote concentration and
improved school performance—in the short run, at least—the cost is high. It
depresses emotional response so that many treated children become lethargic,
withdrawn—"a bit zombieish," Dr. Roberts says.
The drug also causes
insomnia, marked changes in appetite, increased heart rate, and blood
pressure, and/or a suppression of growth hormones. Most troubling of all, in
some susceptible children it triggers Tourette syndrome, an irreversible
malady characterized by multiple tics and generally bizarre behavior. If a
Ritalin patient develops any sort of tic, Dr. Roberts cautions, medication
should be discontinued at once and the physician notified.
10. Teething Remedies. The safest rule is: don’t put any medication
on a baby’s gums. Phenol, paregoric, and benzocaine, three common
ingredients in gum soothers, are all potentially dangerous to infants.
Many home medicine chests
contain preparations that aren’t safe for children. Here are four to be wary
of:
1. Alcohol.
Common children’s medications—teething preparations, decongestants, and
cough syrups—often contain alcohol in concentrations as high as 68 percent.
This is a particular threat to children who may be taking other drugs that
produce serious reactions in combination with alcohol. Parents should read
labels carefully.
Alcohol baths, once standard
for reducing fever, are dangerous. Children sponged with isopropyl alcohol
have died of acute alcohol poisoning.
2. Boric Acid.
This product is toxic when ingested or applied on broken skin and is often
used as an insecticide. It accumulates in the body, so repeated use (in any
way) can cause skin rashes, vomiting, diarrhea, coma, even death. Infants
have died after boric acid was applied to broken skin. Be sure to check
labels and avoid any preparation containing boric acid.
3. Camphor.
A not-so-innocent ingredient in some oils and liniments, camphor is readily
absorbed through the skin and may be carried throughout the body in the
bloodstream. Excessive amounts can cause convulsions, coma, and death.
The FDA has recalled
dangerous products containing 11 percent camphor or more; those with lesser
amounts are of doubtful safety and generally useless. Tragedies have
occurred with distracted parents, reaching for cough medicine, administered
a dose of camphor instead.
4. Hexachlorophene. A phenol-based antiseptic, this drug was
removed from soaps and other products when found to cause brain damage if
applied to the skin of premature infants. Still available by prescription,
it may produce allergic rashes or leave the skin sensitive to sunlight and
is unsafe on burned or broken skin.
Dr. Cynthia Carver, a family
physician and the author of
Patients
Beware! Recommends the following:
-
Don’t ask your child’s doctor for medication. The drugs you get could be useless—and dangerous.
-
When a medicine is prescribed, be sure you know how it should be taken. At whet times? With or without food? Ask about possible side effects, danger signs to watch for.
-
Be sure to tell your doctor about any medication the child is currently taking. Drugs that are safe alone can cause trouble in combination.
-
Follow prescribed dosages exactly, Don’t exceed the amount or frequency of the dose. Be sure to complete the prescribed course of an antibiotic even if all symptoms have disappeared. Never use old antibiotics or give child medications prescribe for someone else.
-
Notify your doctor at once if a child on medication develops a rash, headache, unusual drowsiness, dizziness, stomach, or a marked change in bowel movements.
-
Always ask, "Is there a way to treat this illness or condition without drugs? What kinds of home care—diet, rubs, vaporizer—will help?"
-
Find a pharmacist you can trust to discuss prescribed medications.
-
Read up on prescribed drugs on the Internet. Go to http://www.drugs.com/sfx/ and type in the drug in question for a detailed description of its known side effects.
Dr Fife’s Comments:
The vast majority of illnesses children commonly experience will resolve on
their own without any medical intervention. Bacterial infections can become
life-threatening so antibiotics may be necessary at times. However, viral
and fungal infections do not respond to antibiotics. There is really nothing
the doctor can do for most viral infections and any medication the doctor
prescribes will not shorten the duration of the infection. Antibiotics
should not be taken for a viral infection. They will do little or no good
and may cause a number of troubling side effects.
While medications may be
necessary in some circumstances, often a non-drug solution can be found.
Coconut oil and coconut water have been found to help with many childhood
illnesses. Coconut oil possesses antibacterial, antiviral, and antifungal
properties. It works better for the treatment of diaper rash than any
commercial ointment, and is far safer.
The daily use of coconut oil can
help keep infections at bay. Taken internally it can help fight off systemic
infections. Applied on the skin it can fight surface infections. It is
especially effective for fungal infections such as athlete’s foot, toenail
fungus, and ringworm.
Coconut water is great for
treating dehydration and has proven highly effective in areas hit by
cholera, influenza, and other illnesses that cause severe diarrhea and
dehydration.
Coconut oil, especially when
combined with an appropriate diet, can even be useful, and in many cases
more so than drugs, for the treatment of some more serious conditions such
as epilepsy, autism, learning disability, malnutrition, ADHD, and others.
For a more complete list of
the medicinal uses of coconut oil see my book
Coconut Cures: Preventing and Treating
Common Health Problems with Coconut. For parents with children suffering
from autism or learning disabilities I recommend my book
Stop Autism Now!:
A Parents Guide to Preventing and
Reversing Autism Spectrum Disorders.
Coconut
Cures
by Dr. Bruce Fife
Stop Autism
Now!
by Dr. Bruce Fife
Do you have friends who would like this newsletter? If so, please feel free to share this newsletter with them.
If this newsletter was forwarded to you by a friend and you would like to subscribe, click here.
Copyright © 2016, Bruce Fife. All rights reserved.